

Volume 29, Issue 1 (Winter 2022)
Intern Med Today 2022, 29(1): 34-43 |
Back to browse issues page


![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khorramdel K, Brahmand U, Abolghasemi A, Rashid S, Dashtianeh S, Zare S, et al . Etiology of Hoarding Disorder in Monozygotic and Dizygotic Twins: An Integrated Genetic, Environmental, and Behavioral Model. Intern Med Today 2022; 29 (1) :34-43
URL: http://imtj.gmu.ac.ir/article-1-3974-en.html
URL: http://imtj.gmu.ac.ir/article-1-3974-en.html
Kazem Khorramdel * 

 1, Usha Brahmand2 , Abbas Abolghasemi3 , Sajjad Rashid4 , Soodeh Dashtianeh5 , Shiva Zare6 , Mahshid Mohammadi Mehr7 , Zahra Zafarkhah7
1, Usha Brahmand2 , Abbas Abolghasemi3 , Sajjad Rashid4 , Soodeh Dashtianeh5 , Shiva Zare6 , Mahshid Mohammadi Mehr7 , Zahra Zafarkhah7
1, Usha Brahmand2 , Abbas Abolghasemi3 , Sajjad Rashid4 , Soodeh Dashtianeh5 , Shiva Zare6 , Mahshid Mohammadi Mehr7 , Zahra Zafarkhah7
1- Assistant Professor, Department of Psychology, Fatemiyeh Institute of Higher Education, Shiraz, Iran. , khoramdel.psy@gmail.com
2- Associate Professor, Department of Psychology, CUNY Queens College, USA.
3- Professor, Department of Psychology, University of Guilan, Rasht, Iran.
4- PhD Student in General Surgery, Department of International Education, China Medical University, Shenyang, China.
5- PhD Student of Psychology, Department of Psychology, Marvdasht Branch, Islamic Azad University, Marvdasht, Iran.
6- MA in Psychology, Department of Psychology, Fatemiyeh Institute of Higher Education, Shiraz, Iran.
7- MA Student of Social Psychology, Department of Psychology, Fatemiyeh Institute of Higher Education, Shiraz, Iran.
2- Associate Professor, Department of Psychology, CUNY Queens College, USA.
3- Professor, Department of Psychology, University of Guilan, Rasht, Iran.
4- PhD Student in General Surgery, Department of International Education, China Medical University, Shenyang, China.
5- PhD Student of Psychology, Department of Psychology, Marvdasht Branch, Islamic Azad University, Marvdasht, Iran.
6- MA in Psychology, Department of Psychology, Fatemiyeh Institute of Higher Education, Shiraz, Iran.
7- MA Student of Social Psychology, Department of Psychology, Fatemiyeh Institute of Higher Education, Shiraz, Iran.
Keywords: Dizygotic twins, Environmental and behavioral, Monozygotic twins, Obsessive-compulsive, ِDisorder
Full-Text [PDF 689 kb]
(115 Downloads)
| Abstract (HTML) (291 Views)
Table 1. Mean, standard deviation, minimum, and maximum of age, height, and weight in identical and non-identical groups
Table 2. Mean, standard deviation, minimum, and maximum of the hoarding disorder variable in identical and non-identical groups
Table 3. Variance-covariance matrix and intra-pair correlation coefficient for the hoarding variable in identical and non-identical groups

![]()
Figure 1. Scree plot of the hoarding disorder scores in identical and non-identical groups
Table 4. Results of univariate twin modeling analysis, the best-fitting model for the hoarding variable
H2: Heritability; C2: Shared environmental factor; E2: Non-shared environment; ACI: Akaike Information Criterion; ∆-2LL: -Minus twice the log of the likelihood

Figure 2. Final model of AE for hoarding variable
Full-Text: (28 Views)
Introduction
In the past, the term obsessive-compulsive (OC) spectrum involved numerous disorders that were discussed and revised over time. One of the most important revisions was done in the DSM-5 Research Planning Conference in 2006, based on which it was concluded that the concept of OC spectrum is appropriate for practical, clinical, and diagnostic purposes, and therefore, should not be removed. However, it was suggested that this spectrum should include fewer disorders and there is a need for some reforms. In this conference, the most supported disorders in the OC spectrum were body dysmorphic disorder, hypochondriasis, and trichotillomania. It was also concluded that obsessive hoarding should be categorized as a separate disorder in this spectrum [1].
Uncertainty about the most appropriate classification of hoarding disorder (HD) has had important implications for our understanding of this disorder and has to some extent impeded research efforts in this field. The lack of clear placement in the DSM has led to an underestimation of the importance of HD, inconsistency with regard to an appropriate clinical comparison group in hoarding-related research, difficulties in comparing findings across studies, and misconceptions about the assessment of this disorder [2]. Although still classified as an associated disorder, this disorder is a distinct phenomenon from typical obsessive-compulsive disorder (OCD). Most individuals with HD lack classic OCD symptoms; that is, they are not plagued by intrusive, recurrent thoughts [3].
Hoarding disorder is a syndrome and a debilitating mental disorder [4] that is characterized by collecting objects, storing, and excessive saving that leads to a cluttered living space and significant discomfort or harm. Hoarding is a disorder characterized by persistent difficulty in discarding or parting with possessions regardless of their true value. A person with this disorder has a strong tendency to hoard items and is distressed by throwing them away, which leads to the accumulation of a high degree of clutter [5]. Accumulation of waste, food, and/or animals by an obsessive hoarder can pose a serious threat to personal safety and bring about fire and health hazards. These issues can affect the individual and their family and even engage neighbors and others [6].
Due to ongoing storage, possessions overflow the living space and hinder the daily functioning of life. Severe forms of this behavior can fill the living space and cause health problems [7]. The most frequently stored items are objects and animals. The prevalence of this significant clinical disorder is estimated to be 1.5-2.1% in the general population and may exceed 6% in the elderly [8]. Despite advances in research, much remains unknown about the underlying epidemiology of OCD. Although such information is necessary to map the health services required by this population, only a few studies have been dedicated to investigating OCD from an epidemiological point of view.
Twin studies are a valuable resource for researchers trying to determine whether genetic or environmental factors or both play a role in the development of diseases and disorders [9,10]. This feature is determined based on comparing the degree of concordance of disease symptoms in monozygotic and dizygotic twins. These studies are used to explain the role of genetics and the environment involved in the phenotype of people, and it is considered one of the best methods for identifying genetic markers related to cause and effect factors, which is the foundation of complex psychopathology [11].
Behavioral genetics examines the influence of genes on certain behaviors while also paying attention to the impact and importance of environmental factors on behavior [12]. The findings obtained from genetic studies are in line with family studies, which point to the heritability of obsessive disorder. Univariate twin studies allow us to evaluate the heritability of a trait or disorder. This provides an index of the phenotypic variance ratio in a population, which can be generalized to genetic factors [12,13]. Today, novel genetics science states that genes can lead to some risk factors for humans and show their function at the phenotype level. Phenotype arises from the transcriptional function of genes, and its control plays a crucial role in shaping an individual's reaction to environmental factors and social influences [1].
Relatives often show similar phenotypes for a quantitative trait. The presence of similarity among relatives is a strong indicator of genetic influence on traits that do not demonstrate a straightforward inheritance pattern, including behavioral, physiological, and anatomical features[14,15]. Therefore, genetic effects are examined by comparing phenotypic similarities among relatives, for example, between parents and children, sisters and brothers, and twins. To date, few twin studies have been conducted to investigate the heritability of hoarding symptoms [2]. Studies on gender differences in the prevalence of this disorder have reported different results [16]. There is emerging evidence that a number of factors contribute to OCD symptoms, including genetics, neurocognitive functioning, attachment to possessions, beliefs, avoidance, personality factors, and life events. It is still unknown to what extent each of the etiological factors uniquely contributes to HD [17].
Genetic studies of twins show that HD has a strong genetic component and a complex pattern of inheritance [18]. Evidence also suggests that genetic factors account for approximately half of the phenotypic variance in HD. Obsessive-compulsive phenotype studies have investigated several genes previously involved in OCD. However, no genes have yet been identified as susceptibility genes for HD. Two major limitations have been found in the existing literature: (a) the common use of individuals with OCD rather than samples examining hoarding as a primary phenotype, and (b) non-replication of several existing genetic studies [19].
Longitudinal twin studies of obsessive-compulsive symptoms, a related phenotype, have shown that these symptoms are relatively stable across childhood and adolescence, and that this stability has been largely, however not entirely, explained by genetic factors [20, 21]. A better understanding of the developmental origins of hoarding symptoms in childhood and adolescence has the potential to influence the refinement of diagnostic criteria [22]. Although the etiology of hoarding symptoms is still largely unknown, evidence from twin studies suggests that in adults, genetic factors account for a substantial portion of phenotypic variance, with heritability estimates ranging from 0.36 to 0.49 [23-25]. The results of twin studies conducted at various stages of life indicate the potential for dynamic changes in the etiology of hoarding symptoms, with different genetic and environmental influences over time [22]. This research aimed to determine heritability and the role of environmental factors on HD, using statistical formulas and comparing identical and non-identical twins in Iranian society.
Uncertainty about the most appropriate classification of hoarding disorder (HD) has had important implications for our understanding of this disorder and has to some extent impeded research efforts in this field. The lack of clear placement in the DSM has led to an underestimation of the importance of HD, inconsistency with regard to an appropriate clinical comparison group in hoarding-related research, difficulties in comparing findings across studies, and misconceptions about the assessment of this disorder [2]. Although still classified as an associated disorder, this disorder is a distinct phenomenon from typical obsessive-compulsive disorder (OCD). Most individuals with HD lack classic OCD symptoms; that is, they are not plagued by intrusive, recurrent thoughts [3].
Hoarding disorder is a syndrome and a debilitating mental disorder [4] that is characterized by collecting objects, storing, and excessive saving that leads to a cluttered living space and significant discomfort or harm. Hoarding is a disorder characterized by persistent difficulty in discarding or parting with possessions regardless of their true value. A person with this disorder has a strong tendency to hoard items and is distressed by throwing them away, which leads to the accumulation of a high degree of clutter [5]. Accumulation of waste, food, and/or animals by an obsessive hoarder can pose a serious threat to personal safety and bring about fire and health hazards. These issues can affect the individual and their family and even engage neighbors and others [6].
Due to ongoing storage, possessions overflow the living space and hinder the daily functioning of life. Severe forms of this behavior can fill the living space and cause health problems [7]. The most frequently stored items are objects and animals. The prevalence of this significant clinical disorder is estimated to be 1.5-2.1% in the general population and may exceed 6% in the elderly [8]. Despite advances in research, much remains unknown about the underlying epidemiology of OCD. Although such information is necessary to map the health services required by this population, only a few studies have been dedicated to investigating OCD from an epidemiological point of view.
Twin studies are a valuable resource for researchers trying to determine whether genetic or environmental factors or both play a role in the development of diseases and disorders [9,10]. This feature is determined based on comparing the degree of concordance of disease symptoms in monozygotic and dizygotic twins. These studies are used to explain the role of genetics and the environment involved in the phenotype of people, and it is considered one of the best methods for identifying genetic markers related to cause and effect factors, which is the foundation of complex psychopathology [11].
Behavioral genetics examines the influence of genes on certain behaviors while also paying attention to the impact and importance of environmental factors on behavior [12]. The findings obtained from genetic studies are in line with family studies, which point to the heritability of obsessive disorder. Univariate twin studies allow us to evaluate the heritability of a trait or disorder. This provides an index of the phenotypic variance ratio in a population, which can be generalized to genetic factors [12,13]. Today, novel genetics science states that genes can lead to some risk factors for humans and show their function at the phenotype level. Phenotype arises from the transcriptional function of genes, and its control plays a crucial role in shaping an individual's reaction to environmental factors and social influences [1].
Relatives often show similar phenotypes for a quantitative trait. The presence of similarity among relatives is a strong indicator of genetic influence on traits that do not demonstrate a straightforward inheritance pattern, including behavioral, physiological, and anatomical features[14,15]. Therefore, genetic effects are examined by comparing phenotypic similarities among relatives, for example, between parents and children, sisters and brothers, and twins. To date, few twin studies have been conducted to investigate the heritability of hoarding symptoms [2]. Studies on gender differences in the prevalence of this disorder have reported different results [16]. There is emerging evidence that a number of factors contribute to OCD symptoms, including genetics, neurocognitive functioning, attachment to possessions, beliefs, avoidance, personality factors, and life events. It is still unknown to what extent each of the etiological factors uniquely contributes to HD [17].
Genetic studies of twins show that HD has a strong genetic component and a complex pattern of inheritance [18]. Evidence also suggests that genetic factors account for approximately half of the phenotypic variance in HD. Obsessive-compulsive phenotype studies have investigated several genes previously involved in OCD. However, no genes have yet been identified as susceptibility genes for HD. Two major limitations have been found in the existing literature: (a) the common use of individuals with OCD rather than samples examining hoarding as a primary phenotype, and (b) non-replication of several existing genetic studies [19].
Longitudinal twin studies of obsessive-compulsive symptoms, a related phenotype, have shown that these symptoms are relatively stable across childhood and adolescence, and that this stability has been largely, however not entirely, explained by genetic factors [20, 21]. A better understanding of the developmental origins of hoarding symptoms in childhood and adolescence has the potential to influence the refinement of diagnostic criteria [22]. Although the etiology of hoarding symptoms is still largely unknown, evidence from twin studies suggests that in adults, genetic factors account for a substantial portion of phenotypic variance, with heritability estimates ranging from 0.36 to 0.49 [23-25]. The results of twin studies conducted at various stages of life indicate the potential for dynamic changes in the etiology of hoarding symptoms, with different genetic and environmental influences over time [22]. This research aimed to determine heritability and the role of environmental factors on HD, using statistical formulas and comparing identical and non-identical twins in Iranian society.
Materials and Methods
The current research was conducted using a univariate twin modeling design. The statistical population consisted of all the identical and non-identical twins in Iran in 2019 who were members of the Iranian Twins Association or had health records in the Avicenna Research Institute. The samples were selected using an available sampling method. To this purpose, at the national annual gathering of twins, the twins' health records were chosen randomly. In this study, the sample size was determined using G.Power software. The sample size was determined at 676 individuals consisting of 472 identical and 204 non-identical twins of both genders. In determining whether twins were identical, in addition to using their medical records (if available) and appearance comparison, the self-report similarity questionnaire [26] was utilized, which is a reliable and accurate tool in the field of twin studies. Compared to the DNA test, this questionnaire has shown a specificity and sensitivity of 0.93 to 0.95. The model used to estimate heritability in twins included four effects, namely additive genetics (A), non-additive genetics (D), shared environment (C), and non-shared environment (E).
Implementation method
After consultation with the Iranian Twins Association, in the first step, the link to the questionnaires was sent online to the association's managers, who were requested to distribute them among twins all over Iran (in megacities) so that they could fill them out if they wished. In the second step, on the Twins Day (National Twins Day) event, which was held in Tehran, Iran, with the presence of more than a thousand people, the researchers appeared in the meeting hall and, with prior coordination, distributed paper questionnaires to the twins to complete. Twins were requested to answer simultaneously. After completion, unclear items were removed. Using a self-report questionnaire, identical and non-identical twins were determined. The collected data were entered into the software.
The inclusion criteria of the subjects were having minimum reading and writing literacy and the general qualifications for completing the questionnaire, being proficient in the Persian language, being in the age range of 15-39 years, and being willing to cooperate in the study. On the other hand, the individuals who did not meet the inclusion criteria were excluded from the study. The twins should not have lived apart from each other for more than a month to meet the condition of a shared environment for twin studies. All twins were raised together until the age of 18 years old.
The following tools were used in this research to collect information.
Hoarding Rating Scale-Interview (Tolin, 2010)
This is a 5-item scale that measures the type and intensity of obsessive hoarding disorder in 5 dimensions, namely (1) clutter in the home, (2) difficulty discarding possessions, (3) excessive acquiring of possessions, (4) distress due to hoarding, and (5) functional impairment due to hoarding. The replies are graded on a 9-point Likert scale from 0=not at all to 8=extremely severe. In a study by Frost et al. [27], this instrument showed acceptable reliability and validity for clinical assessment. In the standardized version of this scale in Iran, the results were indicative of the appropriate and desirable psychometric properties of this tool [28]. Moreover, the reliability of this tool was assessed in the present study using Cronbach's alpha coefficient method and obtained at 0.87.
Self-Report of Zygosity (2005)
The Self-Report of Zygosity [29] is a reliable and accurate tool in the field of twin studies and includes two questions:
Implementation method
After consultation with the Iranian Twins Association, in the first step, the link to the questionnaires was sent online to the association's managers, who were requested to distribute them among twins all over Iran (in megacities) so that they could fill them out if they wished. In the second step, on the Twins Day (National Twins Day) event, which was held in Tehran, Iran, with the presence of more than a thousand people, the researchers appeared in the meeting hall and, with prior coordination, distributed paper questionnaires to the twins to complete. Twins were requested to answer simultaneously. After completion, unclear items were removed. Using a self-report questionnaire, identical and non-identical twins were determined. The collected data were entered into the software.
The inclusion criteria of the subjects were having minimum reading and writing literacy and the general qualifications for completing the questionnaire, being proficient in the Persian language, being in the age range of 15-39 years, and being willing to cooperate in the study. On the other hand, the individuals who did not meet the inclusion criteria were excluded from the study. The twins should not have lived apart from each other for more than a month to meet the condition of a shared environment for twin studies. All twins were raised together until the age of 18 years old.
The following tools were used in this research to collect information.
Hoarding Rating Scale-Interview (Tolin, 2010)
This is a 5-item scale that measures the type and intensity of obsessive hoarding disorder in 5 dimensions, namely (1) clutter in the home, (2) difficulty discarding possessions, (3) excessive acquiring of possessions, (4) distress due to hoarding, and (5) functional impairment due to hoarding. The replies are graded on a 9-point Likert scale from 0=not at all to 8=extremely severe. In a study by Frost et al. [27], this instrument showed acceptable reliability and validity for clinical assessment. In the standardized version of this scale in Iran, the results were indicative of the appropriate and desirable psychometric properties of this tool [28]. Moreover, the reliability of this tool was assessed in the present study using Cronbach's alpha coefficient method and obtained at 0.87.
Self-Report of Zygosity (2005)
The Self-Report of Zygosity [29] is a reliable and accurate tool in the field of twin studies and includes two questions:
- Were you and your twin sibling exactly alike since you were a child? Or your resemblance was similar to that of other family members? Yes No
- Did your parents, siblings, or even your teachers mistake you for your twin sibling when you were a child? Yes No
Interpretation
- If both twins answer two questions with yes, or if only one of them answers both questions with yes, they are identical.
- If one or both of them answer both questions with no, they are non-identical.
- If contradictory answers are collected from each twin, they are grouped in the uncertain category. In various studies, few twins were classified in the uncertain category, and meta-analysis studies have classified 7% of the samples as uncertain. In these cases, evaluation is done through direct observation and other physical characteristics. Compared to the DNA test, this questionnaire has shown a specificity and sensitivity of 0.93 to 0.95 [30]. Moreover, the reliability coefficient of Cronbach's alpha was estimated at 0.87 in the present study.
In the current research, SPSS 26 software was used to analyze descriptive data statistics. The correlation between genetic and environmental factors was checked by the maximum likelihood estimation method. For each variable, the concordance correlation coefficient and intra-pair variance-covariance matrices for MZ and DZ twins were extracted using STATA17 software in the form of variance components attributable to genetic factors and shared and non-shared environmental factors. The M-plus 8.3.2 software was used in the analysis of the univariate twin model. Akaike information criterion (AIC) measure of fit index was used as the most important and common index for comparing paired models to select the final model.
Results
The number 676 twins participated in this study, consisting of 472 identical twins (mean age of 24.39 years) and 204 non-identical twins (mean age of 24.13 years) from both genders. Among the identical twins, males accounted for 114 cases (24.2%) and females for 354 subjects (75%), while men and women formed 60 (29.4%) and 142 (69.6%) of the participants in the non-identical group. Among all samples, 6 individuals did not specify their gender.
In both groups, women constituted the largest number of participants, responsible for 75% and 69% of the subjects in the identical and non-identical groups, respectively. The results of descriptive statistics presented on Table 1, showed that the mean age of the two groups was around 24. The youngest participant was 15 years old, whereas the oldest one was 39 years old. The mean scores of the participants' weight in the MZ and DZ groups were approximately 59 and 62 kg, respectively. The mean height in identical and non-identical groups was approximately 164 and 165 m, respectively. The central tendency measures of the HD variable as a general factor are presented in Table 2.
In both groups, women constituted the largest number of participants, responsible for 75% and 69% of the subjects in the identical and non-identical groups, respectively. The results of descriptive statistics presented on Table 1, showed that the mean age of the two groups was around 24. The youngest participant was 15 years old, whereas the oldest one was 39 years old. The mean scores of the participants' weight in the MZ and DZ groups were approximately 59 and 62 kg, respectively. The mean height in identical and non-identical groups was approximately 164 and 165 m, respectively. The central tendency measures of the HD variable as a general factor are presented in Table 2.
Table 1. Mean, standard deviation, minimum, and maximum of age, height, and weight in identical and non-identical groups
| Max | Min | SD | Mean | Variable | Group |
| 39 | 15 | 5.55 | 24.39 | Age | Identical |
| 89 | 40 | 10.83 | 59.29 | Weight | |
| 186 | 150 | 8.18 | 164.90 | Height | |
| 36 | 14 | 5.75 | 24.13 | Age | Non-identical |
| 95 | 40 | 13.17 | 62.55 | Weight | |
| 188 | 150 | 9.88 | 165.70 | Height |
Table 2. Mean, standard deviation, minimum, and maximum of the hoarding disorder variable in identical and non-identical groups
| Max | Min | SD | Mean | Variable | Group |
| 32 | 0 | 8.47 | 10.07 | Twin 1 | Identical |
| 36 | 0 | 8.81 | 10.47 | Twin 2 | |
| 25 | 0 | 6.83 | 9.69 | Twin 1 | Non-identical |
| 25 | 0 | 6.07 | 9.98 | Twin 2 |
According to Table 2, the maximum hoarding scores in the identical group are more than those in the non-identical group, and the mean scores of the identical group are slightly higher than those of the non-identical group.
Table 3 tabulates the concordance correlation coefficient and intra-pair variance-covariance matrices for identical and non-identical twins.
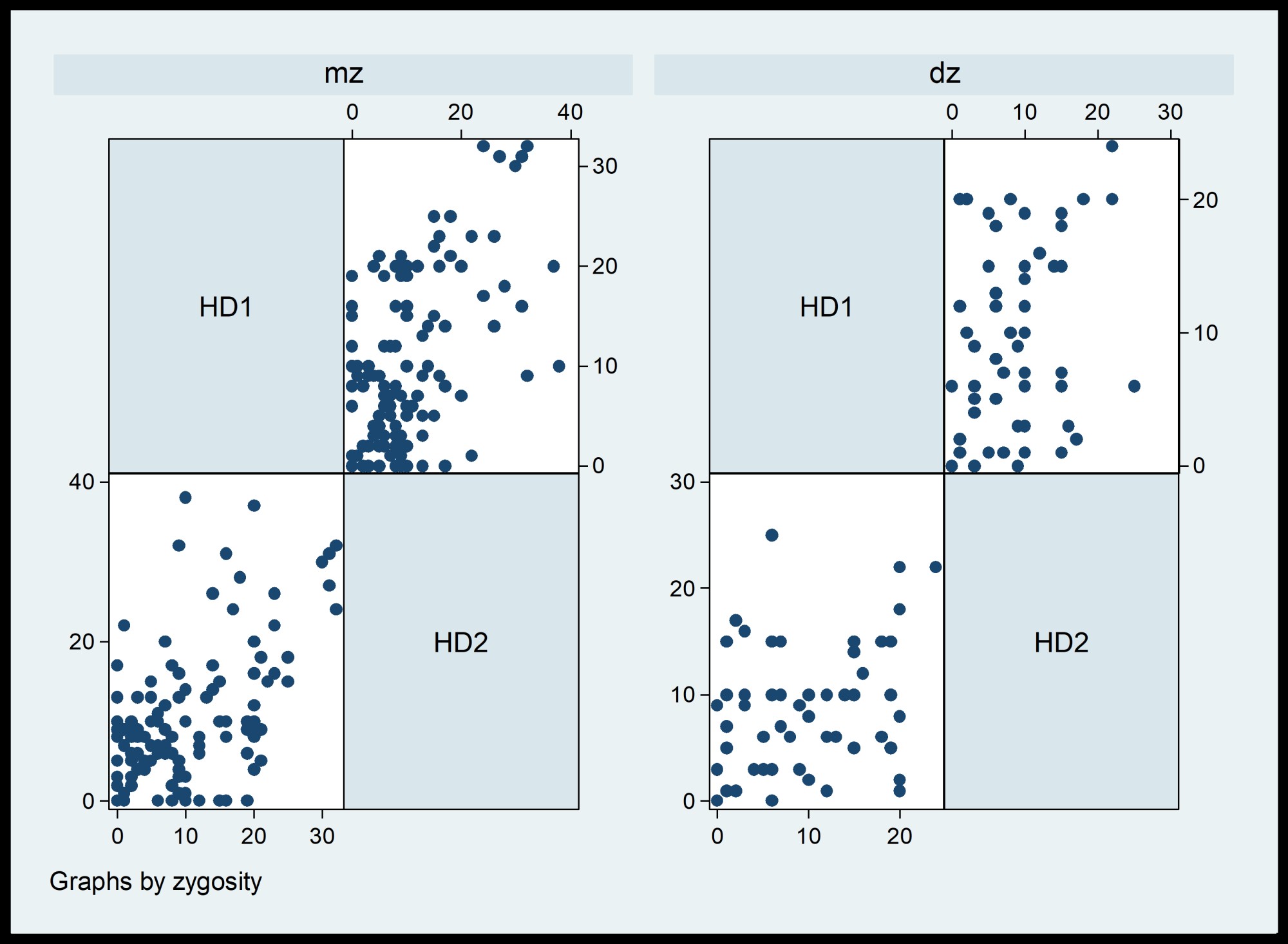
Based on the results of Table 3, the conditions for assumptions of data analysis for running the model are met. In other words, the variance of the DZ group is lower than that of the MZ group. The covariance values in the two groups are less than the variance values. According to the results of the correlation coefficients of the two groups, the correlations of the identical and non-identical groups are 0.58 and 0.26, respectively. This indicates the significant effect of genetics in the occurrence of the phenotype of this variable.
Figure 1 displays the distribution of the HD traits in the two groups and provides similar results to the correlation table.
Table 3 tabulates the concordance correlation coefficient and intra-pair variance-covariance matrices for identical and non-identical twins.
Based on the results of Table 3, the conditions for assumptions of data analysis for running the model are met. In other words, the variance of the DZ group is lower than that of the MZ group. The covariance values in the two groups are less than the variance values. According to the results of the correlation coefficients of the two groups, the correlations of the identical and non-identical groups are 0.58 and 0.26, respectively. This indicates the significant effect of genetics in the occurrence of the phenotype of this variable.
Figure 1 displays the distribution of the HD traits in the two groups and provides similar results to the correlation table.
Table 3. Variance-covariance matrix and intra-pair correlation coefficient for the hoarding variable in identical and non-identical groups
| P | F | TWIN 2 | TWIN 1 | Variable | Group | Hoarding disorder |
| - | 71.79 | Twin 1 | Identical | |||
| 0.09 | 0.71 | 77.71 | 43.77 | Twin 2 | Variance-covariance matrix | |
| - | 46.71 | Twin 1 | Non-identical | |||
| 0.08 | 0.93 | 39.89 | 10.84 | Twin 2 | ||
| - | - | - | 1 | Twin 1 | Identical | |
| - | - | 1 | 0.586 | Twin 2 | Intra-pair correlation coefficient | |
| - | - | - | 1 | Twin 1 | Non-identical | |
| - | - | 1 | 0.261 | Twin 2 |
Figure 1. Scree plot of the hoarding disorder scores in identical and non-identical groups
Table 4. Results of univariate twin modeling analysis, the best-fitting model for the hoarding variable
| Model | ∆df | ∆-2LL | p | AIC | h2 | C2 | E2 |
| ACE | 3 | 19.86 | 0.001 | 13.86 | - | - | - |
| AE | 1 | 1.32 | 0.249 | -0.68 | 0.54 [0.33-0.60] |
0.00 [0.00-0.04] |
0.46 [0.21-0.53] |
| CE | 1 | 1.78 | 0.06 | -0.22 | - | - | - |
| E | 2 | 93.93 | 0.001 | 89.93 | - | - | - |
According to the statistics of the variance-covariance matrix and intra-pair concordance coefficient, the values of additive genetic effect (A), shared environment (C), and non-shared environment (E) were calculated according to the following formula and entered in the final model.
According to the data, the best-fitting model is specified in the second row. As the results show, the AE model is the best-fitting model in the observed data (AIC=-0.68; P˃0.05).
In other words, the additive genetic factor and the non-shared environment explain about 0.54% and 0.46% of the variance of the HD phenotype, respectively. According to the best-fitting model, it is concluded that the additive genetic and non-shared environment comorbidity plays the most important role in the occurrence of HD phenotype, while the role of the shared environment factor is very insignificant.
Along with the model presented in figure 2 fitting results, the figure of the AE model visually shows the significant paths by dark lines:
According to the data, the best-fitting model is specified in the second row. As the results show, the AE model is the best-fitting model in the observed data (AIC=-0.68; P˃0.05).
In other words, the additive genetic factor and the non-shared environment explain about 0.54% and 0.46% of the variance of the HD phenotype, respectively. According to the best-fitting model, it is concluded that the additive genetic and non-shared environment comorbidity plays the most important role in the occurrence of HD phenotype, while the role of the shared environment factor is very insignificant.
Along with the model presented in figure 2 fitting results, the figure of the AE model visually shows the significant paths by dark lines:
|
Twin 2
|
|
Twin 1
|
|
A2
|
|
C1
|
|
C2
|
|
E1
|
|
E2
|
Figure 2. Final model of AE for hoarding variable
Discussion
Our results confirmed the consistent inheritance pattern of this disorder observed in other studies. This population-based study investigated the heritability of symptoms of OCD in twins. The findings showed a significant effect of heritability on obsessive HD symptoms in the studied groups, which supports the research hypothesis proposing that both genetic factors and shared environmental factors are involved in the similarities and differences of HD in twins [15-18]. Therefore, this study contributes to existing research that supports this hypothesis.
The results of a study [31] indicated that identical twins were more similar in terms of obsessive hoarding behavior in comparison to non-identical twins, highlighting the higher effectiveness of genetic factors (A). Moreover, considering environmental factors, the presence of a moderate correlation between identical twins showed the influence of non-shared environmental factors (E). Therefore, based on the findings of this study, shared environmental factors were not able to explain the etiology of obsessive hoarding behavior; consequently, the ACE model, which is representative of the influence of all three factors, was changed to the AE model to indicate the importance and influence of genetic and non-shared environmental factors in the occurrence of obsessive hoarding behavior.
To test this model, the researchers investigated the significant difference in the proposed model by removing factor C, and their results were in line with the initial reports showing the non-effectiveness of factor C. However, the removal of either the A or E factors distorted the model and rendered the entire model meaningless. Therefore, the results of this research were indicative of the 50% effect of additive genetic factor (A) and 50% effect of non-shared environmental factor (E) along with measurement error in the occurrence of obsessive hoarding behavior. It was also found that this disorder was a serious familial disorder.
Another study [32] conducted on 15-year-old twins indicated the existence of a significant pattern of gender differences in the occurrence of obsessive HD. Accordingly, in boys, the additive genetic factor (A) could explain 32% of this disorder, and the rest of the variance was explained by non-shared environmental factor (E) and measurement error (68%). Nevertheless, in girls, shared and non-shared environmental factors (E and C) had the highest level of justification for the occurrence of obsessive HD, and additive genetic factor (A) had an insignificant role. Male identical twins and non-identical twins showed a significant difference in terms of the importance of additive genetic factors, while their female counterparts did not show a significant difference. This suggested the importance of shared environmental factors and the primary effects of the joint family environment in the emergence of obsessive hoarding behavior [33].
In the latest report of twin studies [34] on the spectrum of obsession, the total heritability of HD was found to be 51%. These results confirm the findings of some previous studies highlighting the significance of a family inheritance pattern in the etiology of obsession [35]. These studies emphasize that the family pattern of HD is highly dependent on hereditary, at least in women. Therefore, although environmental factors are also influential, the symptom phenotypes of this disorder manifest in varying ways among different members of the same family [36].
Except for gender-based analysis, which was not included in our study, this finding was very consistent with that of other studies on OCD. Accordingly, this disorder is affected by a moderate heredity and a non-shared environmental role, with the shared environment playing a less significant role. Some molecular genetic studies have attempted to pinpoint the genes associated with Tourette's syndrome in individuals with OCD, a condition that shares considerable similarities with HD. Nevertheless, these findings have thus far yielded conflicting results, and there has not been a study specifically dedicated to examining the genes of vulnerability to HD.
In another study [37], 51 families with 77 pairs of siblings having Gilles de la Tourette syndrome were investigated, and the result was the possible introduction of three gene positions 5q35, 4q34, and 17q25. However, further studies are needed to confirm these results and find other possible and related positions. In a longitudinal research investigating the heritability of the symptoms of OCD in adolescent twins aged 15-18 years, it was discovered that the symptoms persist from adolescence into adulthood, albeit with a slight decrease in heritability over time [38]. This finding was in line with the current research.
Similar results were reported by a meta-analysis of genome-wide association studies of hoarding symptoms in 27,651 individuals [39]. They found that obsessive HD was heritable, with heritability estimates of 26% to 48% for twin groups and 11% for non-related subgroups. Among other studies conducted, we can refer to a study titled "Prevalence and correlates of hoarding behavior and hoarding disorder in children and adolescents" [40]. This research was conducted based on a two-stage evaluation method in two groups of children and adolescents. The final results of their research, which were in agreement with those of our study, showed that the prevalence rate of OCD disorder was 0.98% in children and adolescents, with a higher frequency in females. Furthermore, the presence of any type of psychopathology and female gender were identified as independent correlations of OCD. They also concluded that more than half of the children who were diagnosed with OCD suffered from a psychiatric disorder as well.
In addition to genetic factors, in the present study, non-shared environmental factors accounted for the other half of the variance of HD. This indicates the necessity of identifying the environmental risk factors that increase the probability of developing HD. However, consistent studies that have been conducted exclusively on OCD are not available. Despite this, as the results of previous studies show, there is a strong relationship between stressful life events, age of onset, and severity of HD [41]. In recent studies, loss trauma has also been
mentioned as the prominent environmental factor for the etiology of HD [42].
The results of a study [31] indicated that identical twins were more similar in terms of obsessive hoarding behavior in comparison to non-identical twins, highlighting the higher effectiveness of genetic factors (A). Moreover, considering environmental factors, the presence of a moderate correlation between identical twins showed the influence of non-shared environmental factors (E). Therefore, based on the findings of this study, shared environmental factors were not able to explain the etiology of obsessive hoarding behavior; consequently, the ACE model, which is representative of the influence of all three factors, was changed to the AE model to indicate the importance and influence of genetic and non-shared environmental factors in the occurrence of obsessive hoarding behavior.
To test this model, the researchers investigated the significant difference in the proposed model by removing factor C, and their results were in line with the initial reports showing the non-effectiveness of factor C. However, the removal of either the A or E factors distorted the model and rendered the entire model meaningless. Therefore, the results of this research were indicative of the 50% effect of additive genetic factor (A) and 50% effect of non-shared environmental factor (E) along with measurement error in the occurrence of obsessive hoarding behavior. It was also found that this disorder was a serious familial disorder.
Another study [32] conducted on 15-year-old twins indicated the existence of a significant pattern of gender differences in the occurrence of obsessive HD. Accordingly, in boys, the additive genetic factor (A) could explain 32% of this disorder, and the rest of the variance was explained by non-shared environmental factor (E) and measurement error (68%). Nevertheless, in girls, shared and non-shared environmental factors (E and C) had the highest level of justification for the occurrence of obsessive HD, and additive genetic factor (A) had an insignificant role. Male identical twins and non-identical twins showed a significant difference in terms of the importance of additive genetic factors, while their female counterparts did not show a significant difference. This suggested the importance of shared environmental factors and the primary effects of the joint family environment in the emergence of obsessive hoarding behavior [33].
In the latest report of twin studies [34] on the spectrum of obsession, the total heritability of HD was found to be 51%. These results confirm the findings of some previous studies highlighting the significance of a family inheritance pattern in the etiology of obsession [35]. These studies emphasize that the family pattern of HD is highly dependent on hereditary, at least in women. Therefore, although environmental factors are also influential, the symptom phenotypes of this disorder manifest in varying ways among different members of the same family [36].
Except for gender-based analysis, which was not included in our study, this finding was very consistent with that of other studies on OCD. Accordingly, this disorder is affected by a moderate heredity and a non-shared environmental role, with the shared environment playing a less significant role. Some molecular genetic studies have attempted to pinpoint the genes associated with Tourette's syndrome in individuals with OCD, a condition that shares considerable similarities with HD. Nevertheless, these findings have thus far yielded conflicting results, and there has not been a study specifically dedicated to examining the genes of vulnerability to HD.
In another study [37], 51 families with 77 pairs of siblings having Gilles de la Tourette syndrome were investigated, and the result was the possible introduction of three gene positions 5q35, 4q34, and 17q25. However, further studies are needed to confirm these results and find other possible and related positions. In a longitudinal research investigating the heritability of the symptoms of OCD in adolescent twins aged 15-18 years, it was discovered that the symptoms persist from adolescence into adulthood, albeit with a slight decrease in heritability over time [38]. This finding was in line with the current research.
Similar results were reported by a meta-analysis of genome-wide association studies of hoarding symptoms in 27,651 individuals [39]. They found that obsessive HD was heritable, with heritability estimates of 26% to 48% for twin groups and 11% for non-related subgroups. Among other studies conducted, we can refer to a study titled "Prevalence and correlates of hoarding behavior and hoarding disorder in children and adolescents" [40]. This research was conducted based on a two-stage evaluation method in two groups of children and adolescents. The final results of their research, which were in agreement with those of our study, showed that the prevalence rate of OCD disorder was 0.98% in children and adolescents, with a higher frequency in females. Furthermore, the presence of any type of psychopathology and female gender were identified as independent correlations of OCD. They also concluded that more than half of the children who were diagnosed with OCD suffered from a psychiatric disorder as well.
In addition to genetic factors, in the present study, non-shared environmental factors accounted for the other half of the variance of HD. This indicates the necessity of identifying the environmental risk factors that increase the probability of developing HD. However, consistent studies that have been conducted exclusively on OCD are not available. Despite this, as the results of previous studies show, there is a strong relationship between stressful life events, age of onset, and severity of HD [41]. In recent studies, loss trauma has also been
mentioned as the prominent environmental factor for the etiology of HD [42].
Conclusion
The results of the present study revealed that the correlation rate of the identical group was equal to 0.58, whereas it was 0.26 in the non-identical group. According to the best-fitting model (i.e., AE), the additive genetic factor explained more than 50% of the variance of the HD phenotype, while the other half of the HD variance was explained by the non-shared environmental factor and the error variance. Therefore, the comorbidity pattern of additive genetics and non-shared environment plays the most important role in the occurrence of obsessive phenotype, while the role of shared environment, such as siblings and parenting style, was very small in the etiology of HD.
The main limitation of the present study was related to the medium sample size. The sample size of twin studies usually reaches several thousand people owing to the existence of organized twin registration centers. This issue limits the generalization of our results and does not allow for gender analysis. The statistical methods used in such studies are diverse and relatively complex. Therefore, our results may include calculation errors. The use of self-report tools, a relatively large number of questions, and biased answers were among the other factors that might restrict the generalizability of our results.
It is suggested to carry out twin studies in other mental disorders. Gender and age of onset are two contributing factors that can be tested for their role in the etiology of this disorder in studies with a sufficient sample size, consisting of two genders, and with a wide age range. Referring to the findings, it is recommended to conduct family studies to determine the causal role of non-shared environmental factors in this disorder. These findings can also pave the way for molecular genetic studies in this field. Given the role of non-shared environment factors indicated in our data, implementing preventive measures for at-risk adolescent groups and developing strategies to address environmental factors related to growth could be a way to enhance the well-being of individuals at risk of HD.
The main limitation of the present study was related to the medium sample size. The sample size of twin studies usually reaches several thousand people owing to the existence of organized twin registration centers. This issue limits the generalization of our results and does not allow for gender analysis. The statistical methods used in such studies are diverse and relatively complex. Therefore, our results may include calculation errors. The use of self-report tools, a relatively large number of questions, and biased answers were among the other factors that might restrict the generalizability of our results.
It is suggested to carry out twin studies in other mental disorders. Gender and age of onset are two contributing factors that can be tested for their role in the etiology of this disorder in studies with a sufficient sample size, consisting of two genders, and with a wide age range. Referring to the findings, it is recommended to conduct family studies to determine the causal role of non-shared environmental factors in this disorder. These findings can also pave the way for molecular genetic studies in this field. Given the role of non-shared environment factors indicated in our data, implementing preventive measures for at-risk adolescent groups and developing strategies to address environmental factors related to growth could be a way to enhance the well-being of individuals at risk of HD.
Ethical Considerations
Compliance with ethical guidelinesThe present research was carried out in compliance with all ethical considerations (ethical code IR-FS-IHE-1399-6949) and kept the details and information of the participants confidential.
Authors' contributions
All authors contributed equally to this article.
Funding
This article was a part of the doctoral thesis of the responsible author and was conducted with the financial support of Mohaghegh Ardabili University, Ardabil province, Iran.
Acknowledgments
The authors would like to thank all the participants, officials, and professors who helped us in conducting this research.
Conflicts of interest
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
References
- Leckman JF, Denys D, Simpson HB, Mataix‐Cols D, Hollander E, Saxena S, et al. Obsessive–compulsive disorder: a review of the diagnostic criteria and possible subtypes and dimensional specifiers for DSM‐V. Depress Anxiety. 2010; 27(6): 507–27. [DOI: 10.1002/da.20669] [PMID] [PMCID]
- Grisham JR, Norberg MM. Compulsive hoarding: current controversies and new directions. Dialogues Clin. Neurosci. 2010; 12(2): 233–40. [DOI: 10.31887/DCNS.2010.12.2/jgrishman] [PMID]
- Hombali A, Sagayadevan V, Tan WM, Chong R, Yip HW, Vaingankar J, et al. A narrative synthesis of possible causes and risk factors of hoarding behaviours. Asian journal of Psychiatry. 2019: 42: 104–14. [DOI: 10.1016/j.ajp.2019.04.001] [PMID]
- Marincowitz C, Koen N, Lochner C, Stein DJ. Obsessive–compulsive disorder. InNeurobiology of Brain Disorders. 2023: 825–42. [DOI: 10.1016/B978-0-323-85654-6.00012-5]
- Timpano KR, Exner C, Glaesmer H, Rief W, Keshaviah A, Brähler E, Wilhelm S. The epidemiology of the proposed DSM-5 hoarding disorder: exploration of the acquisition specifier, associated features, and distress [CME]. J Clin Psychiatry. 2011; 72(6): 780–86. [DOI: 10.4088/JCP.10m06380] [PMID]
- Mulligan‐Rabbitt J, O'Connor J, Brien C. “It's not yours. It's mine”: A qualitative study exploring the experience of hoarding. International Journal of Applied Psychoanalytic Studies. 2023; 20(1):120-37. [DOI: 10.1002/aps.1795]
- Nakao T, Kanba S. Pathophysiology and treatment of hoarding disorder. Psychiatry Clin Neurosci. 2019: 73(7): 370–75. [DOI: 10.1111/pcn.12853] [PMID]
- Roane DM, Landers A, Sherratt J, Wilson GS. Hoarding in the elderly: a critical review of the recent literature. Int Psychogeriatr. 2017: 29(7): 1077–84. [DOI: 10.1017/S1041610216002465] [PMID]
- Nordsletten AE, Fernandez de la Cruz L, Aluco E, Alonso P, López-Solà C, Menchón JM, et al. A transcultural study of hoarding disorder: Insights from the United Kingdom, Spain, Japan, and Brazil. Transcult Psychiatry. 2018: 55(2): 261–85. [DOI: 10.1177/1363461518759203] [PMID]
- Bogdanos DP, Smyk DS, Rigopoulou EI, Mytilinaiou MG, Heneghan MA, Selmi C, et al. Twin studies in autoimmune disease: genetics, gender and environment. J Autoimmun. 2012; 38(2-3): J156–69. [DOI: 10.1016/j.jaut.2011.11.003] [PMID]
- Plomin R, DeFries JC, Knopik VS, Neiderhiser JM. Top 10 replicated findings from behavioral genetics. Perspect Psychol Sci. 2016; 11(1): 3–23. [DOI: 10.1177/1745691615617439] [PMID] [PMCID]
- Ayorech Z, Selzam S, Smith-Woolley E, Knopik VS, Neiderhiser JM, DeFries JC, et al. Publication trends over 55 years of behavioral genetic research. Behavior Genetics. 2016; 46(5): 603–07. [DOI: 10.1007/s10519-016-9786-2] [PMID] [PMCID]
- Frost RO, Steketee G, editors. The Oxford handbook of hoarding and acquiring. Oxford University Press. 2014; 7: 19-32. [Link]
- Korner A, Gerull F, Stevenson J, Meares R. Harm avoidance, self-harm, psychic pain, and the borderline personality: life in a “haunted house”. Compr Psychiatry. 2007;48(3):303–08. [DOI: 10.1016/j.comppsych.2007.01.001] [PMID]
- Mathews CA, Delucchi K, Cath DC, Willemsen G, Boomsma DI. Partitioning the etiology of hoarding and obsessive–compulsive symptoms. Psychol Med. 2014; 44(13): 2867–76. [DOI: 10.1017/S0033291714000269] [PMID] [PMCID]
- Hong SI, Bennett D, Rosenheck RA. Gender differences in outcomes of early intervention services for first episode psychosis. Early Interv Psychiatry. 2023; 17(7): 715-23. [DOI: 10.1111/eip.13367] [PMID]
- Dozier ME, Ayers CR. The etiology of hoarding disorder: a review. Psychopathology. 2017; 50(5): 291–96. [DOI: 10.1159/000479235] [PMID]
- Goldstein RG. Challenging the Therapeutic Narrative: Historical and Clinical Perspectives on the Genetics of Behavior. Taylor & Francis. 2023. [Link]
- Hamblin RJ, Lewin AB, Salloum A, Crawford EA, McBride NM, Storch EA. Clinical characteristics and predictors of hoarding in children with anxiety disorders. J Anxiety Disord. 2015; 36: 9–14. [DOI: 10.1016/j.janxdis.2015.07.006] [PMID]
- Krebs G, Waszczuk MA, Zavos HM, Bolton D, Eley TC. Genetic and environmental influences on obsessive-compulsive behaviour across development: a longitudinal twin study. Psychol Med. 2015; 45(7): 1539–49. [DOI:10.1017/S0033291714002761] [PMID]
- van Grootheest DS, Bartels M, Cath DC, Beekman AT, Hudziak JJ, Boomsma DI. Genetic and environmental contributions underlying stability in childhood obsessive-compulsive behavior. Biol Psychiatry. 2007; 61(3): 308–15. [DOI:10.1016/j.biopsych.2006.05.035] [PMID]
- Ivanov VZ, Mataix-Cols D, Serlachius E, Brander G, Elmquist A, Enander J, Rück C. The developmental origins of hoarding disorder in adolescence: a longitudinal clinical interview study following an epidemiological survey. Eur Child Adolesc Psychiatry. 2021; 30: 415-25. [DOI:10.1007/s00787-020-01527-2] [PMID] [PMCID]
- Dozier ME, Ayers CR. The etiology of hoarding disorder: a review. Psychopathology. 2017;50(5):291-6. [DOI:.org/10.1159/000479235]
- Taylor S, Jang KL, Asmundson GJ. Etiology of obsessions and compulsions: a behavioral-genetic analysis. J Abnorm Psychol. 2010; 119(4): 672–82. [DOI:10.1037/a0021132] [PMID]
- Iervolino AC, Perroud N, Fullana MA, Guipponi M, Cherkas L, Collier DA, et al. Prevalence and heritability of compulsive hoarding: a twin study. Am J Psychiatry. 2009; 166(10): 1156–61. [DOI:10.1176/appi.ajp.2009.08121789] [PMID]
- Reed T, Plassman BL, Tanner CM, Dick DM, Rinehart SA, Nichols WC. Verification of self-report of zygosity determined via DNA testing in a subset of the NAS-NRC twin registry 40 years later. Twin Res Hum Genet. 2005; 8(4): 362–67. [DOI: 10.1375%2F1832427054936763] [PMID]
- Frost RO, Tolin DF, Steketee G, Fitch KE, Selbo-Bruns A. Excessive acquisition in hoarding. J Anxiety Disord. 2009; 23(5): 632–39. [DOI: 10.1016/j.janxdis.2009.01.013] [PMID] [PMCID]
- khorramdel K, Rashid S, Barahmand U, Abolghasemi A. Evaluation of the psychometric properties of a Semi- structured Hoarding Rating Scale-Interview (HRS-I) in a Clinical Sample. Ebnesina. 2017; 19(2): 28-35. [Link]
- Hannelius U, Gherman L, Mäkelä VV, Lindstedt A, Zucchelli M, Lagerberg C, Tybring G, Kere J, Lindgren CM. Large-scale zygosity testing using single nucleotide polymorphisms. Twin research and human genetics. 2007;10(4):604-25. [DOI:i.org/10.1375/twin.10.4.604]
- Taylor S, Asmundson GJ, Jang KL. Etiology of obsessive–compulsive symptoms and obsessive–compulsive personality traits: Common genes, mostly different environments. Depress Anxiety. 2011; 28(10): 863–69. [DOI: 10.1002/da.20859] [PMID]
- Nordsletten AE, Monzani B, Fernández de la Cruz L, Iervolino AC, Fullana MA, Harris J, et al. Overlap and specificity of genetic and environmental influences on excessive acquisition and difficulties discarding possessions: Implications for hoarding disorder. Am J Med Genet B Neuropsychiatr Genet. 2013; 162(4): 380–87. [DOI: 10.1002/ajmg.b.32149] [PMID]
- Ivanov VZ, Mataix-Cols D, Serlachius E, Lichtenstein P, Anckarsäter H, Chang Z, Gumpert CH, et al. Prevalence, comorbidity and heritability of hoarding symptoms in adolescence: a population based twin study in 15-year olds. PloS one. 2013; 8(7): e69140. [DOI: 10.1371/journal.pone.0069140] [PMID]
- Arnold PD, Sicard T, Burroughs E, Richter MA, Kennedy JL. Glutamate transporter gene SLC1A1 associated with obsessive-compulsive disorder. Archives of general psychiatry. 2006; 63(7): 769-76. [DOI: 10.1001/archpsyc.63.7.769] [PMID]
- Monzani B, Rijsdijk F, Harris J, Mataix-Cols D. The structure of genetic and environmental risk factors for dimensional representations of DSM-5 obsessive-compulsive spectrum disorders. JAMA psychiatry. 2014; 71(2): 182-89. [DOI: 10.1001/jamapsychiatry.2013.3524] [PMID]
- Schulze TG, Hedeker D, Zandi P, Rietschel M, McMahon FJ. What is familial about familial bipolar disorder?: Resemblance among relatives across a broad spectrum of phenotypic characteristics. Archives of General Psychiatry. 2006; 63(12): 1368-76. [DOI: 10.1001/archpsyc.63.12.1368] [PMID]
- Samuels JF, Bienvenu OJ, Grados MA, Cullen B, Riddle MA, Liang KY, Eaton WW, Nestadt G. Prevalence and correlates of hoarding behavior in a community-based sample. Behaviour research and therapy. 2008; 46(7): 836–44. [ DOI: 10.1016/j.brat.2008.04.004] [PMID] [PMCID]
- Mathews CA, Nievergelt CM, Azzam A, Garrido H, Chavira DA, Wessel J, et al. Heritability and clinical features of multigenerational families with obsessive‐compulsive disorder and hoarding. Am J Med Genet B Neuropsychiatr Genet. 2007; 144B(2): 174–82. [DOI: 10.1002/ajmg.b.30370] [PMID]
- Ivanov VZ, Nordsletten A, Mataix-Cols D, Serlachius E, Lichtenstein P, Lundström S, Magnusson PK, Kuja-Halkola R, Rück C. Heritability of hoarding symptoms across adolescence and young adulthood: A longitudinal twin study. PloS one. 2017; 12(6): e0179541. [DOI: 10.1371/journal.pone.0179541] [PMID]
- Strom NI, Smit DJ, Silzer T, Iyegbe C, Burton CL, Pool R, Lemire M, Crowley JJ, Hottenga JJ, Ivanov VZ, Larsson H. Meta-analysis of genome-wide association studies of hoarding symptoms in 27,651 individuals. Transl Psychiatry. 2022; 12(1): 479. [DOI: 10.1038/s41398-022-02248-7] [PMID] [PMCID]
- Akıncı MA, Turan B, Esin İS, Dursun OB. Prevalence and correlates of hoarding behavior and hoarding disorder in children and adolescents. Eur Child Adolesc Psychiatry. 2022; 31(10): 1623–34. [DOI: 10.1007/s00787-021-01847-x] [PMID]
- Cromer KR, Schmidt NB, Murphy DL. Do traumatic events influence the clinical expression of compulsive hoarding?. Behav Res Ther. 2007; 45(11): 2581–92. [DOI: 10.1016/j.brat.2007.06.005] [PMID]
- Landau D, Iervolino AC, Pertusa A, Santo S, Singh S, Mataix-Cols D. Stressful life events and material deprivation in hoarding disorder. Journal of anxiety disorders. 2011; 25(2):192-202. [DOI: 10.1016/j.janxdis.2010.09.002] [PMID]
Type of Study: Original |
Subject:
Mental Health
Received: 2023/04/3 | Accepted: 2023/05/24 | Published: 2023/06/19
Received: 2023/04/3 | Accepted: 2023/05/24 | Published: 2023/06/19
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |